What causes this condition in the first place? We see more of it in females than males at any given community road race. Even the leanest and fastest post puberty females have some if it around the buttocks and thighs. This post looks at a 2010 study that searched for genetic causes of cellulite in females. This post follows a previous post making the case for red light reversing fibrosis in keloid scars via induction of a poorly understood collagen protease called PRss35. Fibrotic scars involve an interplay between TGFβ and HIF1α. Near infrared lasers inserted into the cellulite are the only proven therapy for improving the appearance of cellulite. The science behind what might what cause cellulite suggests non invasive red light therapy might help too on levels that extend beyond the cosmetic.
Causes of cellulite

- Toxin accumulation. This toxin would be lipo polysaccharide of GI bacteria and the TLR4 receptor
- Enlarged fat cells, estrogen receptors and other genes associated with lipid metabolism of course.!
- Poor circulation, nitric oxide synthase, of course. Red light helps here.
- Fibrosis of connective tissue. an interplay between TGFβ and HIF1α covered in the previous post
- Water retention, the renin, angiotensin aldosterone system of course
Genetic predispositions to cellulite, Emanuele 2010
The Geroldi Lab of Department of Internal Medicine and Medical Therapeutics, University of Pavia, Pavia, Italy compared the genomes of 200 lean females seeking cellulite treatment with that of 200 lean females without cellulite. The controls were age, BMI, region, and such matched.
The Major Allele Frequency (MAF) is the proportion of the most common allele (copy of a gene) at a specific genetic locus in a population, expressed as a fraction or percentage. It is calculated by dividing the number of copies of the major allele by the total number of allele copies at that locus in the population. We have two copies of most genes on each chromosome, except the Y in most individuals. Single Nucleotide Polymorphisms (SNP) are variations in coding and non-coding parts of our genomes. The reduction in the cost of genetic sequencing has resulted in an effort to correlate these minute variations with conditions. There is even a website called SNPedia.com that describes these variations and their association with conditions.. A polymorphism need not be in the protein coding part of a gene to have an impact on the functioning of the individual. Each of these SNPs is assigned a Reference SNP number, or rs for short. Using SNP to predict whom will get a condition is an enduring fad. The SNPs Emanuele examined fall in the realm of possible causes of cellulite. Only two made the cut as predictors. The following discusses the findings of Emanuele 2010 as they relate to five possible causes of cellulite.
Cellulite comes from toxin accumulation
SNPs in The Toll-like receptor #4 (TLR4) did not make the cut as a single predictor. Lipopolysaccharide from Gram Negative bacteria is considered a primary ligand of this receptor that mediates the immune response to invaders. The possibility is that multiple SNPs and environmental factors determine who gets cellulite
Cellulite is an inflammatory condition?
A London based clinic called Lipotherapeia makes the claim that cellulite fibrose fat, is pro inflammatory like visceral fat. This clinic usesblue light, 630 and 830 nm red NIR for a variety of conditions including cellulite. in 2023 Kruglicov and Scherer published a review that gives a nice cartoon image of cellulite. This particular review stressed the inflammatory nature of cellulite. Note the presence of MUSE cell. See Conti 2020 for more discussion of MUSE cells and some MRI and scanning electron microscope images of cellulite. Wikipedia authors have assembled an interesting page on MUSE cells that goes beyond the peer reviewed papers on this post. MUSE cells are puripotent stem cells that can be isolated from adipose tissue.
TLR4 Leaky gut and cellulite? Kruglikov and Scherer 2023
This is a very nice review that goes into the extracellular matric of the structures that hold our gluteal femoral adipose tissue into structures known as cellulite. The Lipotherapeia clinic stresses that cellulite is not to be confused with sub cutaneous fat. The concept of MUSE cells, noncancerous, stress‐tolerant pluripotent human mesenchymal stromal cells (hMSC). These cells can differentiate into adipocytes by exposure to different factors. They also express estrogen receptors and are known to play an important role in tissue repair and regeneration. In butt/thigh white adipose tissue prone to cellulite, these cells constitute about 85%–90% of the whole mesenchymal stromal cell population. The number of MUSE cells directly with the clinical grade of cellulite.The TLR4 ligand, lipopolysaccharide, is proposed to come from a leaky gut. Their comment ” It is well established that overloading of adipose tissue with salts leads to activation of the renin–angiotensin–aldosterone system and release of Ang II, which induces activation of inflammatory cytokines and enhances adipogenesis/lipogenesis.” Why must LPS come from the gut? Fig 4 of Conti , a transmission electron microscope image of human cellulite shows sweat glands in close proximity with adipocytes and some extracellular vesicles that might be means of communication. What if bacteria part of the skin microbiome are the source of LPS? Fig 2 of Kruglikov and Scherer, the concept in cartoon form, opens the question of whether bacteria living in a sweat gland could seed cellulite. Note the inclusion of matrix metallo proteases degrading collagen and other matrix that cause fat to herniate into the dermis.
Enlarged fat cells,Conti 2010
SNPs of estrogen receptors and many fat handling enzymes failed to make the cut as single predictors of cellulite in the female volunteers of the Emanuele 2010 study. An interesting link exists between both estrogen receptors and mitochondria. The thought remains that multiple SNPs may contribute to cellulite.
The Conti 2010 study favored all of the above mechanisms. Estrogen receptors were part of the model. Cellulite was isolated from 10 women (23–45 years old, with a BMI ranging between 24 and 27) Other experiments were performed with 10 gluteo femoral samples from cadavers (5 male, 5 female, 25–45 years old, with a BMI ranging between 24 and 27). Mesenchymal Stem Cells and of Multilineage Differentiating Stress Enduring Cells (MUSE) were isolated from cellulite.
“Mesenchymal stem cells are rich in estrogen receptors and are recruited after stress stimuli, represented by oxidative stress, matrix remodeling, reactive oxygen species production, as demonstrated by proteomic analysis (Figure 7). The proteomic analysis of cellulite and of MUSE cells, isolated from cellulite specimens, showed the presence of estrogens receptors on the multilineage differentiating stress enduring cells membranes , demonstrating the pivotal role of these cells in the cellulite development. According to the previous theories about cellulite progression, our results recognize the importance of estrogenic stimulation. Our hypothesis on MUSE role, is that these cells, after estrogenic stimuli, could activate all the bio chemical cascades of prostaglandins production, cyclooxygenases expression, and of stimulation of matrix metallo proteinases and elastases. A schematic summary is reported in Figure 8, in which we try to clarify the development of cellulite. The recruitment of MUSE, bringing the estrogens receptor, induces the deep remodeling of the dermis and the activation of pro-inflammatory pathways.”
“Results: light and electron microscopy of the cellulite affected area showed a morphology completely different from the other usual adipose depots. In cellulite affected tissues, sweat glands associated with adipocytes were found. In particular, there were vesicles in the extracellular matrix, indicating a crosstalk between the two different components. Proteomic analysis showed that adipose tissue affected by cellulite is characterized by high degree of oxidative stress and by remodeling phenomena. Conclusions: The novel aspects of this study are the peculiar morphology of adipose tissue affected by cellulite, which could influence the surgical procedures finalized to the reduction of dimpling, based on the collagen fibers cutting. The second novel aspect is the role played by the mesenchymal stem cells isolated from stromal vascular fraction of adipose tissue affected by cellulite.”
Poor Circulation Oliveira-Paula 2016
The nitric oxide synthase 3 polymorphism Glu298Asp or E298D(or G894T) did not make the cut as a predictor of cellulite, Emanuele, 2010. The Oliveira-Paula review covered this and other NOS3 SNPs These are some links to informative images in the review.
- How NOS3 works goes with red light and PEMF. Note the increase in intracellular Ca2+ and other cofactors involved.
- The functional group anatomy of NOS3 makes it clear red light absorbing heme groups are part of nitric oxide synthesis
- The NOS3 gene anatomy figure addresses not only the genetic variations mentioned by Emanuele 2010 but also other thingsthat might be going on in a woman’s life. Transforming growth factor β1 (TGF-β1), a homodimeric peptide that plays an important role in the fibrosis, increases NOS3 promoter activity.
- . Functional mechanisms of NOS3 polymorphisms is a figure showing how complicated these SNPs.
There’s more to Oliveira-Paula 2016, much of it hving to do with hypertension.
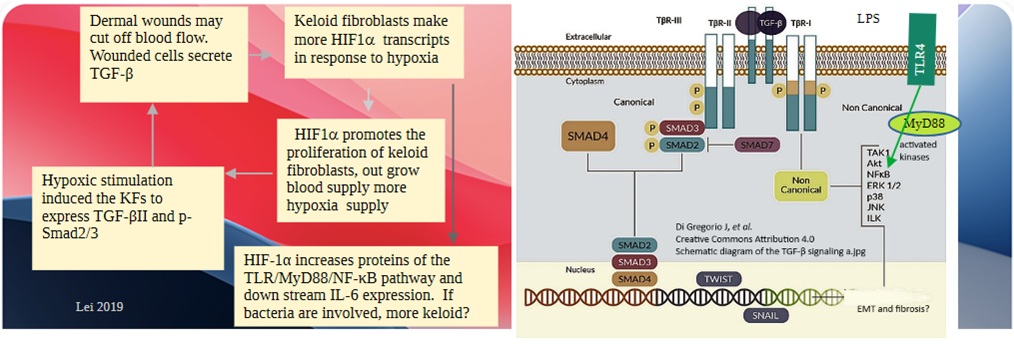
Fibrosis of connective tissue, TGFβ and HIF1α
Alone, TGFB SNPs failed to predict cellulite, Emamuele 2010. On the other hand, the HIF1A rs11549465 genotype CC was found in 85% of women without cellulite versus 72.5% with those women with cellulite.
Pro582 is considered the wildtype. Pro582 is not one of the prolines that gets hydroxylated in normoxia. According to UniProt entry Q16665 the proline hydoxylation sites are Pro564 and Pro402. There are some phosphorylation sites at Ser576 and Ser589. Back to
“Transforming growth factor β1 (TGF-β1) levels influence many cellular, immunologic and pathologic processes. Activator protein 1 (AP1) and hypoxia are key regulators of TGF-β1 expression levels. The common TGFB1 promoter SNP c.−1347C > T (−509C-T, rs1800469) has been linked to a nearly twofold difference in plasma levels among individuals and with risk, progression, and outcome of numerous diseases. We demonstrate exclusive in vitro and in vivo recruitment of AP1 containing JunD to −1347C. This study also is the first to demonstrate hypoxia inducible factor 1 (HIF-1) binding to the TGFB1 promoter. HIF-1 was found to associate with both −1347C and −1347T and compete with AP1 for binding to −1347C. Reporter constructs demonstrate that expression differences between −1347C and −1347T are due to selective AP1 recruitment to the TGFB1 promoter. As AP1 is known to down-regulate transcription of other genes, we suggest that the molecular mechanism for the difference in TGF-β1 plasma levels linked to −1347 is due to transcriptional suppression by AP1 binding to −1347C. These data should aid in our understanding of the association of the −1347 SNP with the pathogenesis of certain TGF-β1-related diseases.” Shah 2006
An imagine is emerging in which three genes, TGFB, HIF1, and NOS3, can work together for fibrosis of connective tissue. Underactive NOS3 leads to hypoxia, which activates HIF1A, which increases TGFB transcripts…
Water retention
The ACE1 rs1799752 genotype was found in 16% of women with cellulie and in 26% of those without it. Just one D allele was found in 62.3% with cellulite and 50.8 % without it.
ACE1 is part of the renin-angiotensin-aldosterone system (RAAS, While issues with the RAAS might influence the appearance of cellulite, this post will stick to concepts that are influenced by red light and/or PEMF. The RAAS, ACE1, and water retention:
- The juxtamedullary apparatus in the macula densa of the kidney detects changes in flow of renal filtrate. A protease called renin is released.
- Renin cleaves a ten amino acid peptide from the pro-hormone angiotensinogen. This peptide is called angiotensin I.
- The protease Angiotensin Converting Enzyme (ACE) cleaves two amino acids off angiotensin I to yield the octapeptide angiotensin II.
- Agiotensin II is a potent vasoconstrictor that increases blood pressure.
- Angiotensin II works on the kidneys to increase water and sodium absorption.
- Angiotensin II acts on the adrenal cortex to release the steroid hormone aldosterone. Aldosterone increases water and sodium retention.
- Angiotensin also triggers the release of anti-diuretic hormone (ADH) from the pituitary gland,
rs1799752 is one of four SNPs representing perhaps the best studied ACE (angiotensin I converting enzyme) SNP. It is actually not a single nucleotide polymorphism at all; instead, it is an insertion/deletion of an Alu repetitive element in an intron of the ACE gene. Alleles containing the insertion are called “I” alleles, and “D” alleles lack the repetitive element. The renin-angiotensin-aldosterone system RAAS tends to l!!!ead to fluid retention and hypertension.
If athe cause of woman’s cellulite has to due with SNPs of the ACE1 gene and subsequent water retention, she best see her health care provider to determine if she has hypertension and is a good candidate for ACE inhibitors.
Clinical trials, cellulite improvement by NIR heating
All genetic and environmental causes of cellulite notwithstanding, these NIR trials were involved in inserting a cannula into the offending tissue and heating. These trials were performed with NIR YAG (yttrium alumina garnet) lasers inserted subcutaneously. The Introduction if Truit 2014 states the use of YAG lasers for other FDA approved indications. All of these studies involve follow up six months to a year later. DiBernardo (2011, 2013, 2016) is the invention of the technique in a private clinic. Katz 2013 is a very similar study as is Sasaki 2013. Truitt 2013 only used a 1064 nm YAG laser. Bagatin (2013) used NIR and reflective compression stockings in which blinding was to which leg was getting the NIR. All of the sub cutaneous YAG laser studies resulted in significant improvements in appearance.
It would be totally wrong to say that red and NIR LED lights have been proven to improve the appearance of cellulite. Let’s take the claim of the Lipotherapeia Clinic seriously, that cellulite is more than a cosmetic problem but rather a source of pro-inflammatory adipokines that is just as dangerous as visceral fat. It sould be noted that this clinic also uses radio frequency PEMF and ultrasound in addition to the blue, red, and NIR . lights.
- If toxins can also come from the sweat glands, might anti-microbial blue light help too?
- Emanuele 2010 polymorphism in the estrogen receptors did not alone predict which lean women would get cellulite. there is a curious interplay between the mitochondria and estrogen receptors.
- Nitric oxide improves poor circulation via nitric oxide production. If a woman has poorer circulation due to a NOS3 polymorphism, could red light therapy tip the balance?
- Red light to minimize the vicious cycle of TGFβ and HIF1α in fibrotic scars has been covered in a previous post. Can red light cause the secretion of the collagen degrading protease PRss35? If it can, does decrease in collagen make the cellulite less pro-inflammatory?
Red and NIR just for health
A single cause of cellulite was not found in the peer reviewed literature. Lack of good circulation seems to be major theme, Perhaps NOS3 cofactor supplements would be part of this “for health theme. From functional group anatomy of NOS3 we have: nicotinamide adenine dinucleotide phosphate (niacin), flavin mononucleotide (riboflavin), and flavin adenine dinucleotide (riboflavin), heme, zinc, tetrahydrobiopterin, and L-arginine.
References
- Bagatin E, Miot HA, Soares JL, Sanudo A, et al. (2013) Long-wave infrared radiation reflected by compression stockings in the treatment of cellulite: a clinical double-blind, randomized and controlled study. Int J Cosmet Sci 2013;35:502–9. PubMed
- Conti G, Zingaretti N, Amuso D, Dai Prè E, Brandi J, Cecconi D, Manfredi M, Marengo E, Boschi F, Riccio M, Amore R, Iorio EL, Busato A, De Francesco F, Riccio V, Parodi PC, Vaienti L, Sbarbati A. (2020) Proteomic and Ultrastructural Analysis of Cellulite-New Findings on an Old Topic. Int J Mol Sci. 2020 Mar 18;21(6):2077. PMC free paper
- DiBernardo BE. (2011) Treatment of cellulite using a 1440-nm pulsed laser with one-year follow-up. Aesthet Surg J 2011;31:328–41. PubMed
- DiBernardo B, Sasaki G, Katz BE, Hunstad JP, et al.(2013) A multicenter study for a single, three-step laser treatment for cellulite using a 1440-nm Nd:YAG laser, a novel side-firing fiber, and a temperature-sensing cannula. Aesthet Surg J 2013;33:576–84. PubMed
- DiBernardo BE, Sasaki GH, Katz BE, Hunstad JP, et al. (2016)A multicenter study for cellulite treatment using a 1440-nm Nd:YAG wavelength laser with side-firing fiber. Aesthet Surg J 2016;36:335–43.
PMC free article - Emanuele E, Bertona M, Geroldi D. (2010) A multilocus candidate approach identifies ACE and HIF1A as susceptibility genes for cellulite. J Eur Acad Dermatol Venereol. 2010 Aug;24(8):930-5. Sci-Hub free paper
- Katz B. (2013) Quantitative and qualitative evaluation of the efficacy of a 1440 nm Nd:YAG laser with novel bi-directional optical fiber in the treatment of cellulite as measured by 3-dimensional surface imaging. J Drugs Dermatol 2013;12:1224–30. PubMed
- Kruglikov IL, Scherer PE. (2023) Pathophysiology of cellulite: Possible in volvePMC free paper
- Oliveira-Paula GH, Lacchini R, Tanus-Santos JE. (2016) Endothelial nitric oxide synthase: From biochemistry and gene structure to clinical implications of NOS3 polymorphisms. Gene. 2016 Jan 10;575(2 Pt 3):584-99. PMC free paper
- Sasaki GH. (2013) Single treatment of grades II and III cellulite using a minimally invasive 1,440-nm pulsed Nd:YAG laser and side-firing fiber: an institutional review board-approved study with a 24-month follow-up period. Aesthet Plast Surg 2013;37:1073–89. PubMed
- Shah R, Hurley CK, Posch PE. (2006) A molecular mechanism for the differential regulation of TGF-beta1 expression due to the common SNP -509C-T (c. -1347C > T). Hum Genet. 2006 Nov;120(4):461-9. PubMed
- Truitt A, Elkeeb L, Ortiz A, Saedi N, et al.(2012) Evaluation of a long pulsed 1064-nm Nd:YAG laser for improvement in appearance of cellulite. J Cosmet Laser Ther 2012;14:139–44. PubMed
Leave a Reply